You've rested it. You've stretched it. You may have bought new shoes, changed your desk setup, tried heat, tried ice, and told yourself it would settle down on its own. Yet the heel still bites when you get out of bed, the elbow still complains every time you lift a bag, or the shoulder keeps catching when you reach overhead.
That's usually the point where people start searching for answers and run into a wall of confusing terms. One of them is shockwave therapy. It sounds intense, a bit technical, and easy to dismiss as just another trendy machine treatment. In practice, it's far more grounded than that.
For the right problem, shockwave therapy is a non-invasive treatment used to stimulate repair in stubborn musculoskeletal tissues. It has been used in musculoskeletal care for decades, and a major review found positive outcomes in 88.5% (23 of 26) of radial ESWT randomised controlled trials and 81.5% (66 of 81) of focused ESWT randomised controlled trials indexed in PEDro, while also identifying a commonly used protocol of 3 treatment sessions, 1 week apart, with 2,000 impulses per session in this review of ESWT evidence and treatment protocols.
Table of Contents
- Tired of Persistent Pain? An Introduction to Shockwave Therapy
- What Exactly Is Shockwave Therapy
- How Shockwave Therapy Promotes Natural Healing
- Common Conditions That Respond Well to Shockwave Therapy
- What to Expect During and After Your Session
- Weighing the Benefits Risks and Suitability
- Integrating Shockwave Therapy into Your Osteopathic Care
Tired of Persistent Pain? An Introduction to Shockwave Therapy
Persistent pain has a particular way of wearing people down. It's not always dramatic. Often it's the same sharp heel pain each morning, the same sore Achilles after a walk, or the same tendon ache that flares every time you return to exercise.
By the time someone asks about shockwave, they're usually not looking for a miracle. They want a next step that makes sense. They want to know why the tissue hasn't settled and whether there's a treatment that does more than dull the discomfort for a few hours.
That's where extracorporeal shockwave therapy, often shortened to ESWT, comes in. In plain language, it's a way of delivering targeted mechanical energy into irritated or slow-to-heal tissue without surgery or injections. The aim isn't to “blast away” pain. The aim is to stimulate a healing response in tissue that has become stubborn, overloaded, or biologically quiet.
Practical rule: Shockwave tends to make the most sense when pain has hung around, the diagnosis is reasonably clear, and simpler measures haven't been enough.
It also helps to place it in context. Shockwave isn't new, and it isn't fringe. It has been part of musculoskeletal care for decades. That matters because many patients come in assuming it's an experimental add-on. It's better understood as a modern tool used within standard allied-health and rehabilitation settings for selected conditions.
For people with long-running tendon pain or plantar fasciopathy, that distinction is important. If your tissue has stopped responding to rest alone, the answer often isn't more rest. It may be a more precise form of loading and stimulation, delivered in a controlled way.
What Exactly Is Shockwave Therapy
Shockwave therapy is a hands-on, machine-delivered treatment that sends short bursts of mechanical energy into injured or irritated tissue through the skin. The area is covered with gel, a handpiece is placed over the target tissue, and a series of pulses is applied without needles or surgery.
For patients, the practical question is usually simple. What makes this different from the other machines used in rehab?
The answer is that shockwave is designed to create a controlled mechanical stimulus in tissue that has stopped responding well to usual care. It is not the same as therapeutic ultrasound, TENS, or a massage device. It works more like a precise tap to the healing system, aimed at a specific structure rather than the whole region.
That distinction matters in osteopathic practice. I do not use shockwave as a stand-alone gadget for any sore spot. It works best when the painful structure is reasonably clear, the irritability pattern makes sense, and the treatment is paired with the broader things that help tissue recover, such as load management, joint motion, strength work, and a plan that fits daily life.
Radial and focused are not the same
Patients often hear these terms and assume they mean the same treatment. They do not.
Radial shockwave spreads energy over a broader area and is commonly used for more superficial tissues.
Focused shockwave concentrates energy more precisely and can be used to reach deeper or more specific targets.
A simple comparison helps:
- Radial treatment works more like a spray pattern across an area
- Focused treatment works more like a spotlight on a defined point
Neither type is automatically better. The better choice depends on what tissue is involved, how deep it sits, how sensitive the area is, and what the treatment is trying to achieve. The International Society for Medical Shockwave Treatment provides a useful overview of these differences in its explanation of radial and focused shockwave therapy.
What shockwave is used for
In practice, shockwave is usually reserved for specific musculoskeletal problems rather than vague pain that moves around without a clear pattern.
Common examples include:
- Plantar fasciopathy with ongoing heel pain
- Tendinopathies such as Achilles, patellar, or tennis elbow pain
- Calcific shoulder pain in selected cases
- Some bone-healing applications in specialist medical settings
In Australia, this is one reason a proper assessment matters. People often arrive asking whether shockwave is covered by Medicare or whether they should book a package of sessions straight away. The more useful starting point is whether the diagnosis is one that tends to respond to shockwave, and whether the tissue still needs better loading, a footwear change, or hands-on osteopathic care around the painful area.
Shockwave is a targeted treatment for selected conditions. It is not a general fix for every ache, and it should make sense within the whole treatment plan.
How Shockwave Therapy Promotes Natural Healing
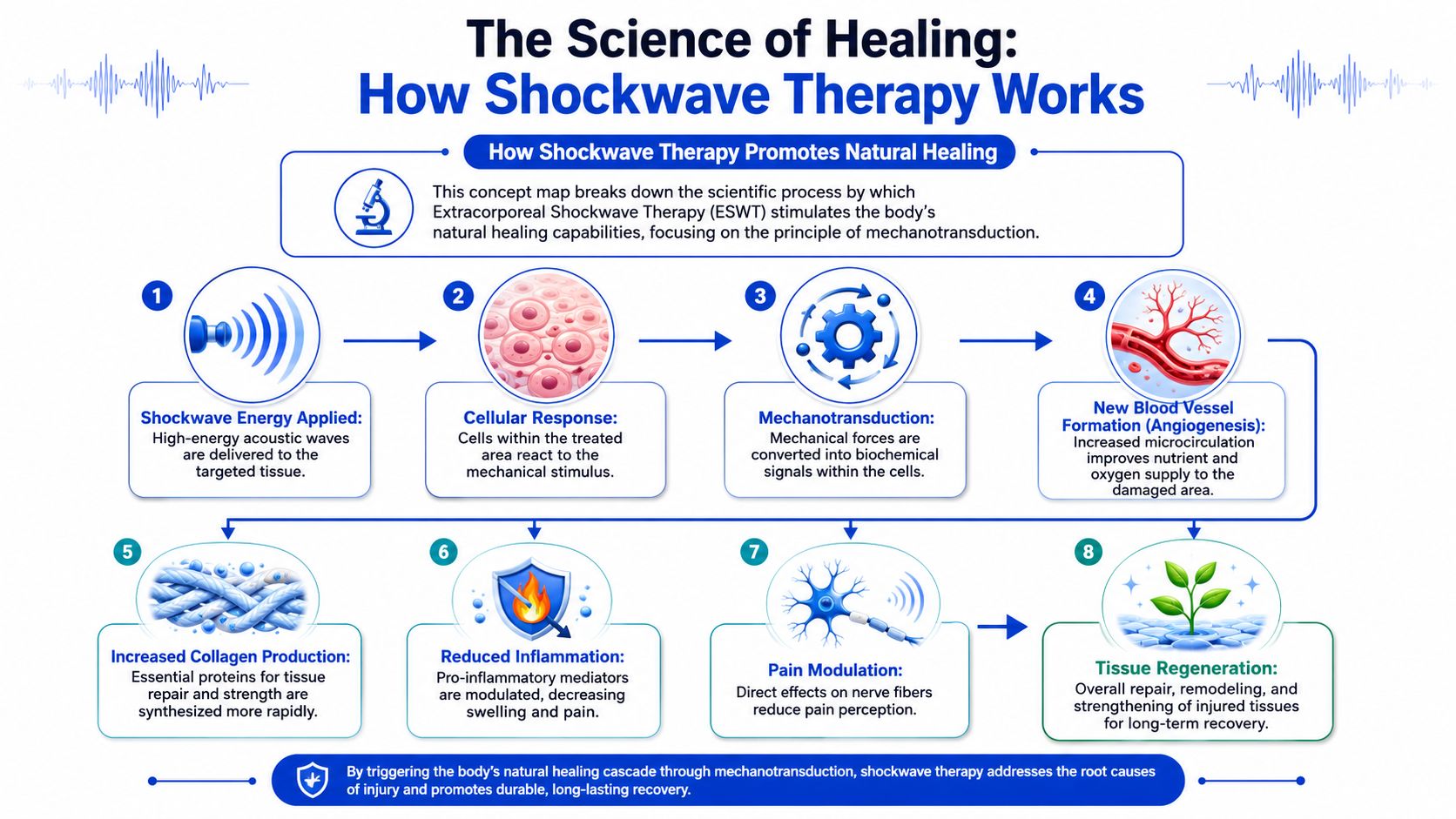
Shockwave therapy works through mechanotransduction. That's the biological process where mechanical force is converted into chemical signals inside cells. It sounds technical, but the core idea is simple. The tissue feels a mechanical input, and the body responds by changing its healing behaviour.
A therapeutic signal, not a cover-up
The reason this matters is that shockwave isn't mainly trying to hide symptoms. Its intended job is to trigger repair signalling. According to this review of ESWT mechanisms and musculoskeletal applications, mechanical loading from the shockwave is converted into biochemical signalling that increases neovascularization, fibroblast activity, collagen synthesis, and osteoprogenitor differentiation, while also modulating inflammatory mediators and pain pathways.
That long sentence translates well into everyday language:
- New blood vessel formation can improve the local healing environment
- Fibroblast activity helps support tissue repair
- Collagen synthesis matters because collagen gives tendons and similar tissues their structure
- Pain pathway modulation may reduce how irritable the area feels
This is why some people describe the treatment as “waking the area up”. Chronic tendon tissue often isn't torn in the dramatic way people imagine. It may be disorganised, overloaded, and not repairing efficiently. Shockwave gives that tissue a clear mechanical message.
Why chronic tissue sometimes needs a nudge
A sore tendon that has lingered for months often behaves differently from an acute injury. Rest may calm it for a while, but full recovery stalls because the tissue hasn't rebuilt tolerance well. That's why a passive approach alone often disappoints.
Shockwave can fit into that gap because it provides brief high-energy mechanical stress that encourages repair signalling. In musculoskeletal care, this is why ESWT is commonly used for chronic tendinopathies, plantar fasciopathy, greater trochanteric pain syndrome, and delayed bone healing or nonunion in appropriate settings, as outlined in the same mechanism review above.
The key idea is simple. Shockwave doesn't replace the body's healing response. It tries to prompt it.
That's also why treatment usually works best when paired with the basics: good diagnosis, sensible load management, and a rehabilitation plan that matches the person in front of you.
Common Conditions That Respond Well to Shockwave Therapy
The people most likely to ask “what is shockwave therapy?” are often dealing with a familiar list of problems. Heel pain that won't settle. Tennis elbow that keeps returning. A shoulder that feels pinchy and weak for months. A hip that aches when lying on that side at night.
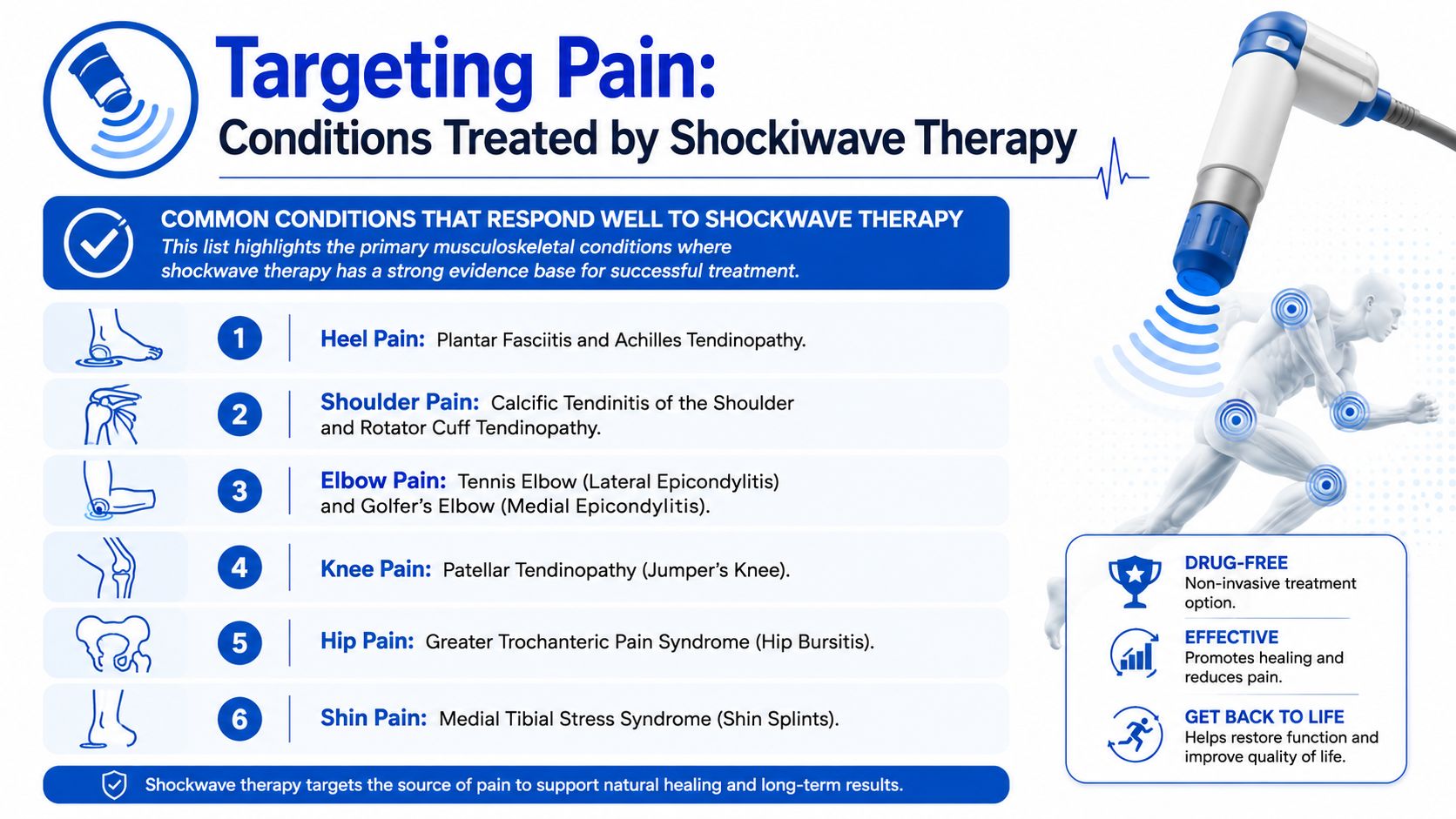
Foot, ankle and lower limb pain
Plantar fasciopathy is one of the most common reasons people explore shockwave. The classic story is pain under the heel with first steps in the morning or after sitting. When symptoms become persistent, the tissue often needs more than stretching alone.
Achilles tendinopathy can also respond well when the tendon remains sore, stiff, and reactive over time. This is especially common in runners, active walkers, and people who increase activity too quickly after a quiet period.
Patellar tendon pain and other long-standing lower limb tendon problems may also be considered when loading programmes haven't been enough on their own.
For a visual example of the sort of musculoskeletal assessment that often sits around these decisions, this clinical treatment image from an allied-health setting captures the broader context well.
{kind=link}
Elbow, shoulder and hip problems
At the elbow, tennis elbow and golfer's elbow are common presentations. These problems often linger because gripping, lifting, typing, gym work, and even household jobs keep loading the irritated tendon.
At the shoulder, shockwave is often discussed for calcific tendinopathy and some chronic tendon-related pain patterns. It isn't a blanket answer for every shoulder complaint. A shoulder can hurt because of stiffness, referred neck pain, rotator cuff tendon overload, bursa irritation, or osteoarthritis. The diagnosis has to come first.
At the hip, greater trochanteric pain syndrome is another condition often considered. People usually describe this as pain on the outside of the hip, worse with lying on that side, stairs, or longer walks.
Mayo Clinic notes that the evidence base is expanding, and that nuance matters in real practice because patients need help understanding not just what the treatment is used for, but also when it is appropriate and when something else may be better suited, as discussed in Mayo Clinic's clinician update on shockwave treatment.
What to Expect During and After Your Session
One reason people delay treatment is simple uncertainty. If you don't know what the machine feels like, how long the appointment takes, or whether you'll be able to walk out normally afterwards, it's easy to put it off.
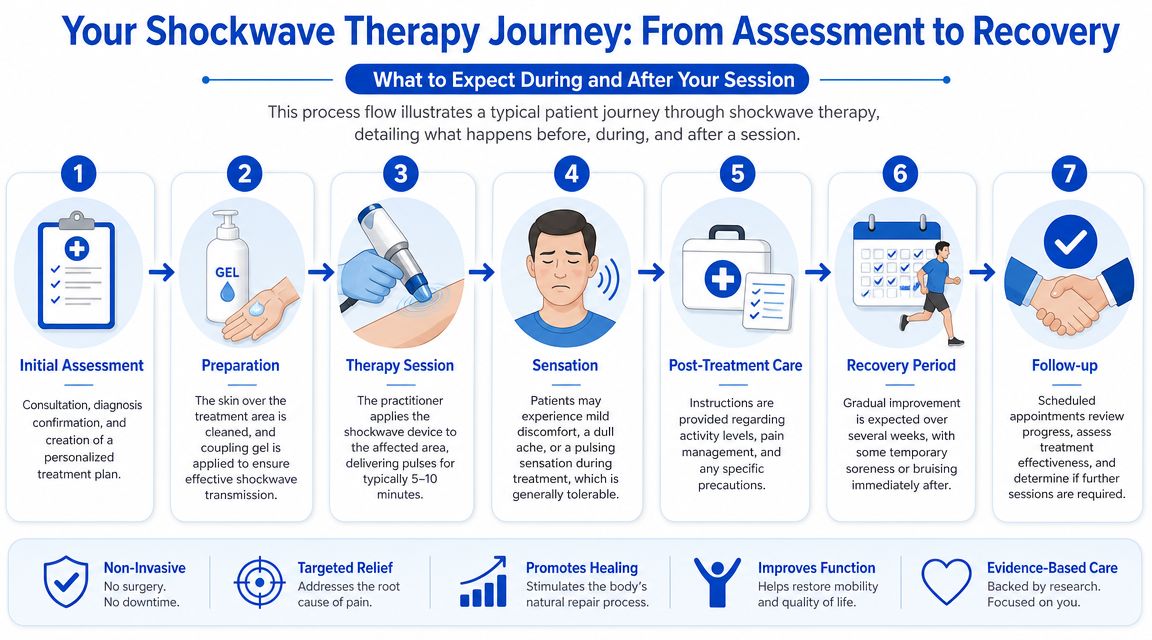
During the appointment
A proper session starts with assessment, not with switching on the machine straight away. The clinician needs to confirm what structure is likely driving the pain, whether shockwave fits the diagnosis, and whether there are reasons not to proceed.
Once the area is identified, gel is placed on the skin and the handpiece is applied over the target tissue. The pulses usually feel like a fast tapping or repetitive thudding sensation. Some people describe it as sharp over very tender points. Others find it more odd than painful.
The treatment itself is usually brief, and many patients tolerate it well once they know what to expect. If you'd like to see the device and treatment style in action, this short video demonstration of shockwave therapy gives a useful visual reference.
Most people don't need downtime afterwards, but they do need realistic expectations. It can be uncomfortable during treatment, and improvement often builds over time rather than arriving the same day.
After the session
Afterwards, the area may feel worked on. Mild soreness, localised pain, redness, or bruising can happen. Recent expert-facing guidance also describes minimal activity restrictions and common minor effects such as erythema, bruising, and localised pain in Ohio State Wexner Medical Center's shockwave therapy overview.
That doesn't mean “do anything you want”. It usually means sensible activity modification rather than complete rest.
A common pattern after treatment looks like this:
- Same day: The area may feel tender or stirred up.
- Next few days: Symptoms can fluctuate. This doesn't automatically mean the treatment has failed.
- Following weeks: Progress is judged by pain reduction, improved tolerance to loading, and better function.
Many clinicians use shockwave as an adjunct, not a stand-alone fix. That's an important distinction. If the tissue is being overloaded by training errors, poor capacity, footwear issues, or movement habits, those factors still need attention.
Weighing the Benefits Risks and Suitability
You have had heel, shoulder, or tendon pain for months. Exercises have helped a bit, rest has helped a bit, and you are now weighing whether shockwave is worth trying. This is usually the point where a clear discussion matters more than a sales pitch.

Shockwave therapy has real strengths. It also has limits. In practice, the right question is not whether shockwave is good or bad. It is whether it fits your diagnosis, your stage of healing, your goals, and your tolerance for a treatment that can be briefly uncomfortable.
Where shockwave can help
One reason people consider shockwave is simple. It is non-invasive. There is no incision, no injection, and in an osteopathic clinic it can often be added to a broader treatment plan without disrupting work or family life.
It is also focused. That matters for stubborn local problems such as plantar fasciopathy, Achilles or gluteal tendinopathy, some calcific shoulder presentations, and selected chronic soft-tissue pain states where the painful structure has been clearly identified. In those cases, a targeted mechanical stimulus may make more sense than repeating generic massage or resting indefinitely.
From a patient point of view, the practical upsides are usually these:
- It is drug-free. That appeals to people who want to reduce reliance on pain relief where possible.
- Appointments are usually short. The shockwave part does not take long.
- It can sit alongside rehab. Exercise, load management, footwear changes, and hands-on care still matter.
- It can be useful when progress has stalled. That is often when people ask about it.
In Australian practice, another practical question comes up quickly. Is it covered? Shockwave provided in private allied-health settings is commonly an out-of-pocket service. Medicare does not usually fund routine shockwave treatment in the way patients often hope, although broader care may intersect with GP management plans or specialist referrals depending on the condition and setting. That is worth checking before starting a course, especially if you are comparing it with an injection or specialist review. This medical graphic comparing where cortisone may fit in treatment decisions can help frame that discussion.
{kind=link}
When shockwave is a poor fit
Suitability starts with diagnosis.
If the pain comes from the spine, a nerve, an inflammatory flare, or a joint problem rather than the tendon or fascia being treated, shockwave may add cost and discomfort without solving the main issue. I am cautious with it when the assessment is unclear, because a precise treatment still misses the mark if it is aimed at the wrong tissue.
There are also situations where shockwave should be avoided or delayed pending medical advice. Pregnancy, active infection, and clotting disorders are commonly treated as contraindications or reasons for further review. Patients with a recent significant injury, unexplained swelling, marked night pain, or symptoms that suggest something more than a routine musculoskeletal problem also need proper assessment first.
Then there is the question of timing. Shockwave is often better suited to persistent problems than very fresh injuries. A tissue that is acutely irritable may need load reduction, clearer diagnosis, or calmer rehabilitation before a stronger local stimulus is useful.
The trade-offs patients should know
The main downside is not mystery. It is tolerance.
Treatment can be uncomfortable while it is being applied, especially over sore tendons or the heel. Some patients are happy to put up with that because the sessions are brief and the problem has dragged on for months. Others decide the discomfort is not worth it, or they prefer to start with exercise and manual care alone. Both are reasonable.
Cost matters too. A course often involves more than one session, so the decision is rarely about a single appointment. In an osteopathic setting, I usually discuss whether the expected benefit justifies that cost, and whether the same budget might be better spent on diagnosis, exercise guidance, footwear changes, or another referral.
A good decision is usually quite grounded. What exactly are we treating? How confident are we in the diagnosis? Have simpler measures been tried properly? Is the person likely to follow through with the rehab that should sit around the shockwave?
Shockwave can be a useful tool. It is not a shortcut, and it is not the answer to every persistent pain problem. The best candidates are usually people with a clear diagnosis, a chronic local tissue issue, realistic expectations, and a treatment plan that looks at the whole body rather than the sore spot alone.
Integrating Shockwave Therapy into Your Osteopathic Care
Shockwave is at its best when it sits inside a broader plan. In osteopathic practice, that matters because pain rarely exists in isolation. A sore heel changes the way you walk. A painful shoulder alters the neck, upper back, and ribcage. A persistent tendon problem often changes confidence and movement long before it changes scan findings.
How it fits with hands-on care
A whole-body osteopathic approach asks two questions at once. First, what tissue is painful? Second, what is keeping that tissue irritated?
That's where shockwave can complement gentle manual care rather than compete with it. Hands-on treatment may help improve movement, reduce protective tension, and settle surrounding joints or soft tissues. Shockwave may then be used to target the stubborn tendon or fascia that needs a stronger local stimulus.
In practical terms, a plan might include:
- Assessment of the painful structure and the nearby joints affecting load
- Gentle osteopathic treatment to improve mobility and reduce guarding
- Shockwave therapy where a chronic local tissue problem fits the picture
- Exercise and load advice so the tissue builds tolerance instead of flaring again
For patients comparing options, the most useful question isn't “Which treatment is best overall?” It's “Which treatment best matches my diagnosis, stage of healing, and goals?” This rehabilitation equipment image from a clinical setting reflects that wider rehab mindset well.
{kind=link}
Medicare and practical Australian questions
In Australia, people often ask whether Medicare covers osteopathic care or adjunct treatments such as shockwave. The answer depends on your circumstances and care plan. If you have a Chronic Disease Management plan arranged through your GP, you may be eligible for a Medicare rebate for approved allied-health services. The rebate rules can change, and eligibility is individual, so it's worth discussing the details with your GP and your clinic directly.
Patients also ask whether shockwave replaces exercise, injections, or physiotherapy. Usually, it doesn't replace everything. It fills a particular role.
| Treatment | Mechanism | Best For | Considerations |
|---|---|---|---|
| Shockwave therapy | Mechanical stimulus intended to trigger tissue repair signalling | Chronic tendon pain, plantar fasciopathy, selected persistent musculoskeletal conditions | Non-invasive, targeted, may cause brief discomfort, best with clear diagnosis |
| Corticosteroid injection | Anti-inflammatory medication delivered to a specific area | Situations where short-term symptom reduction is a priority and a medical practitioner considers it appropriate | May reduce pain, but doesn't automatically build tissue capacity or address movement factors |
| Physiotherapy or osteopathic rehab | Exercise prescription, movement retraining, manual techniques, load management | Broad range of musculoskeletal pain and recovery stages | Often foundational. Progress depends on consistency and the right diagnosis |
| Watchful waiting and self-management | Relative rest, pacing, home exercises, footwear or ergonomic changes | Milder or early presentations | Appropriate for some cases, but persistent pain usually needs reassessment if it's not improving |
Shockwave therapy makes the most sense when it's chosen carefully, explained clearly, and integrated into care that still respects the whole person rather than chasing one sore spot.
If you're dealing with heel pain, tendon pain, shoulder pain, or another stubborn musculoskeletal issue and want clear guidance on whether shockwave fits your situation, Bayside Osteopathic Health offers gentle, individualized osteopathic care with practical advice on treatment options, rehabilitation, and Medicare pathways where applicable.