If you're dealing with back pain that never quite settles, neck stiffness that flares after a workday, or joint pain that has slowly become part of everyday life, it's easy to feel stuck. Many people cycle through short GP visits, pain relief, stretches from memory, and the hope that things will calm down on their own. Sometimes they do. Often, they don't.
What usually makes chronic pain harder isn't only the pain itself. It's the lack of a clear plan. You know something needs ongoing attention, but the system can feel full of jargon, referrals, item numbers, and uncertainty about cost. That's where Medicare chronic disease management can make a real difference. Used properly, it gives you a structured way to organise care for a condition that has been, or is likely to be, present for the longer term.
For people considering osteopathic care for ongoing musculoskeletal pain, this matters. A chronic condition plan can create a practical link between your GP, your allied health providers, and the hands-on support you may need to move better and hurt less.
Table of Contents
- Living with Chronic Pain and Seeking Solutions
- What Is a Medicare Chronic Disease Management Plan
- Are You Eligible for a Chronic Disease Management Plan
- Covered Services and Potential Costs
- Your Step-by-Step Guide to Getting a CDM Plan
- How Bayside Osteopathic Health Supports Your Care Plan
- Frequently Asked Questions About CDM Plans
Living with Chronic Pain and Seeking Solutions
A familiar pattern goes like this. Your lower back has been sore for months. Some weeks it's manageable, then one long drive, one bad sleep, or one busy week at your desk brings it all back. You adjust your activity, cancel a walk, lean more on pain relief, and tell yourself you'll deal with it properly later.
The same happens with neck pain, shoulder tightness, arthritis, or persistent hip discomfort. The problem isn't just that the pain lingers. It's that you start managing your life around it. You turn down plans, move more carefully, and stop trusting your body.
For many patients, the turning point comes when they realise they don't need to approach chronic pain as a series of isolated flare-ups. They need coordinated care. Medicare chronic disease management exists for exactly that reason. It's designed for conditions that have lasted, or are likely to last, for the longer term, including musculoskeletal problems such as arthritis.
In Australia, approximately 4 million people, or 16% of the population, used a GP Chronic Disease Management Plan in 2020 to 2021 to coordinate care for chronic conditions, including musculoskeletal disorders like arthritis, according to the Australian Institute of Health and Welfare summary on GP Chronic Disease Management Plan use.
What this changes for a patient
A chronic disease management plan isn't magic, and it doesn't remove the work of getting better. What it does is replace guesswork with structure.
That means:
- A clearer pathway: Your GP documents the condition being managed and the type of support that may help.
- Better coordination: Allied health care isn't left as a vague suggestion. It becomes part of a formal plan.
- A more proactive approach: You're no longer waiting until things get worse before seeking help.
Chronic pain usually responds best when care is organised, reviewed, and matched to your actual day-to-day limits.
If headaches are part of the picture along with neck tension, even a simple visual explanation of symptom patterns can help you put words around what you're experiencing, such as this illustrated tension headache overview.
{kind=link}
Why patients often delay using it
People often assume these plans are only for severe illness, older age, or very complex medical situations. That's a mistake. If you've had persistent pain, recurring stiffness, reduced mobility, or an arthritic condition that's affecting your function, it's worth asking the question.
The key shift is this. Instead of asking, "How do I get through this week?" you start asking, "How do I manage this properly over time?" That's where the system starts working for you.
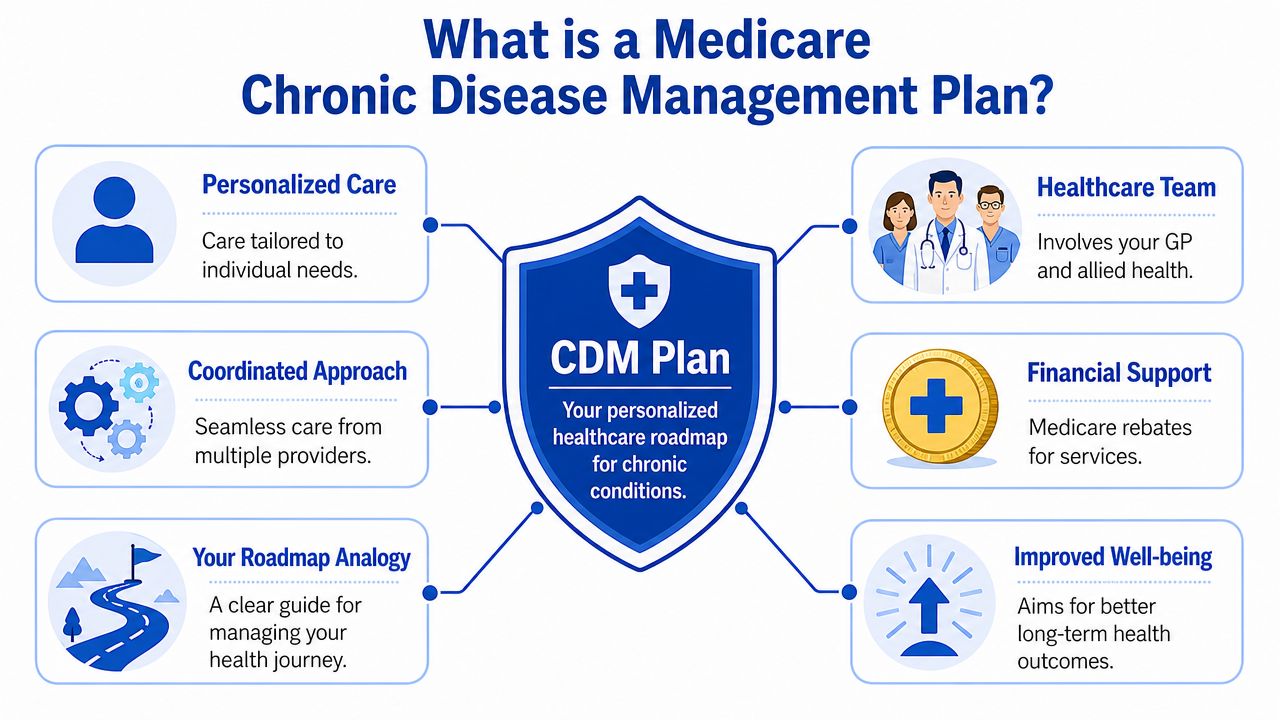
What Is a Medicare Chronic Disease Management Plan
Think of a Medicare chronic disease management plan as a healthcare roadmap. Your GP uses it to set out what condition is being managed, what your main care needs are, and which allied health services may help. It isn't the same as a routine appointment for a script or a quick check-in. It's a formal plan for ongoing, coordinated care.
That distinction matters. Chronic pain care often falls apart when each appointment stands alone. One person tells you to rest, another says to strengthen, another suggests imaging, and nobody ties it together. A proper management plan creates a shared direction.
The name changed in 2025
From 1 July 2025, the GP Chronic Condition Management Plan (GPCCMP) replaced the older GP Management Plan and Team Care Arrangements, and the change removed the previous requirement for mandatory consultation with two other providers to set up the plan, as outlined by the Australian Government information on upcoming chronic disease management changes.
For patients, the main practical effect is that the setup process is simpler. You still need your GP to assess your needs and document the plan properly, but there are fewer administrative hurdles.
What a plan usually does
A good plan turns vague concerns into concrete management goals. For someone with chronic musculoskeletal pain, that may include reducing pain with movement, improving walking tolerance, managing stiffness, or supporting function at work and home.
It also helps answer practical questions such as:
- What condition is being managed
- Why allied health is clinically relevant
- Who is involved in your care
- When the plan should be reviewed
Practical rule: If your pain has become a repeating pattern rather than a short-term injury, you probably need a management strategy, not another one-off appointment.
Why this matters for osteopathic care
For a patient considering osteopathy, the plan can create a formal pathway into care that focuses on movement, mobility, and non-drug support. That's especially helpful when pain isn't only about one sore spot. Many chronic presentations involve posture, guarded movement, stiffness, poor load tolerance, sleep disruption, and fear of aggravation.
A management plan doesn't guarantee that every treatment style will suit every person. It does create the structure that lets your GP and allied health providers work from the same page. That alone often reduces confusion and delay.
Are You Eligible for a Chronic Disease Management Plan
The central rule is straightforward. You may be eligible if you have a medical condition that has been present, or is likely to be present, for at least six months. That includes musculoskeletal conditions such as arthritis, and your GP must decide that allied health services would benefit the management of that condition within the formal care plan, as explained in this overview of chronic disease management plan eligibility.
Musculoskeletal problems that often fit the criteria
Patients are often surprised by how relevant this is to everyday pain problems seen in clinic settings. You don't need to be dealing with one dramatic diagnosis for the plan to be worth discussing.
Examples that may fit include:
- Chronic low back pain: Especially when it keeps recurring or limits sitting, lifting, walking, or sleep.
- Osteoarthritis: Joint pain and stiffness affecting knees, hips, hands, spine, or other areas.
- Persistent neck pain: Ongoing restriction, tension, or pain linked to desk work, driving, or repeated flare-ups.
- Sciatica or nerve-related leg pain: When symptoms have continued beyond an acute episode.
- Shoulder pain that lingers: Reduced range, pain reaching overhead, or pain disturbing sleep.
What your GP is actually deciding
Eligibility isn't only about the diagnosis. Your GP is also deciding whether allied health care is likely to help manage the condition in a meaningful way.
That usually comes down to questions like these:
- Is the problem ongoing?
- Is it affecting function or quality of life?
- Would structured support from an allied health provider help?
If the answer is yes, a care plan discussion makes sense.
The six-month rule doesn't mean you have to wait in pain for six months before speaking up. It means the condition is chronic in nature, or likely to be.
What doesn't work well
Patients sometimes ask for a plan as if it's a discount voucher for any treatment they want. That's not how the system works. The referral needs to relate to managing the chronic condition identified by your GP.
It also helps to avoid being vague in your appointment. Saying "I've just been a bit sore" often doesn't capture the reality. Saying "I've had neck pain for months, it affects driving and sleep, and I think allied health treatment could help me manage it better" gives your GP something specific to assess.
Covered Services and Potential Costs
The part most patients want to understand is simple. Under this system, eligible patients can access up to five Medicare-subsidised allied health services per calendar year under their plan. Depending on your condition and referral, that may include osteopathy, physiotherapy, podiatry, dietetics, psychology, and other allied health care relevant to the condition being managed.
This doesn't mean five sessions with every provider. It means five subsidised allied health services in total, to be used in line with your GP's referral and care plan.
What Medicare support often looks like
In 2019, Medicare paid nearly $1 billion for chronic disease management services, and approximately 99% of these services were bulk billed, according to the AIHW chapter on spending for chronic disease management services.
That tells you two useful things. First, the program is widely used. Second, bulk billing is common within the broader system. Even so, it doesn't guarantee that every allied health clinic bulk bills every appointment.
The rebate commonly discussed for eligible allied health services is $63.40 per session, for up to five rebates annually for eligible providers under the plan. Whether you have an out-of-pocket cost depends on the clinic's fee structure.
Bulk billed versus gap payment
A simple way to understand it:
- Bulk billed appointment: The provider accepts the Medicare rebate as full payment for that service.
- Gap payment: The provider charges above the rebate amount, and you pay the difference.
Before booking, ask the clinic two direct questions:
- Do you accept chronic disease management referrals?
- Is there a gap fee for these appointments?
If you're managing arthritis or joint stiffness, this arthritis and joint mobility image reflects the kind of functional issue many patients are trying to improve through allied health care.
{kind=link}
Commonly Subsidised Allied Health Services Under a CDM Plan
| Allied Health Service | How It Can Help Your Chronic Condition |
|---|---|
| Osteopathy | Hands-on care aimed at improving mobility, easing muscular tension, and supporting movement in chronic musculoskeletal conditions |
| Physiotherapy | Exercise-based and manual support for strength, movement control, rehabilitation, and pain management |
| Podiatry | Support for foot pain, gait issues, pressure problems, and lower limb mechanics |
| Dietetics | Nutritional guidance where weight, inflammation, diabetes, or other health factors affect long-term management |
| Psychology | Support when pain, stress, mood, sleep, or coping are part of the broader condition picture |
Ask about cost before your first visit, not at the reception desk after treatment. That conversation is easier and clearer when you have it upfront.
The trade-off patients should understand
The rebate helps, but it won't always cover the full fee. The stronger value often comes from using those subsidised visits strategically. For chronic pain, that may mean combining assessment, hands-on treatment, movement advice, and a home plan rather than expecting five appointments to solve a long-standing problem on their own.
Your Step-by-Step Guide to Getting a CDM Plan
If the system feels bureaucratic, the easiest way to handle it is to follow a sequence. Most problems happen when patients book the wrong appointment type, arrive unprepared, or assume the referral happens automatically.
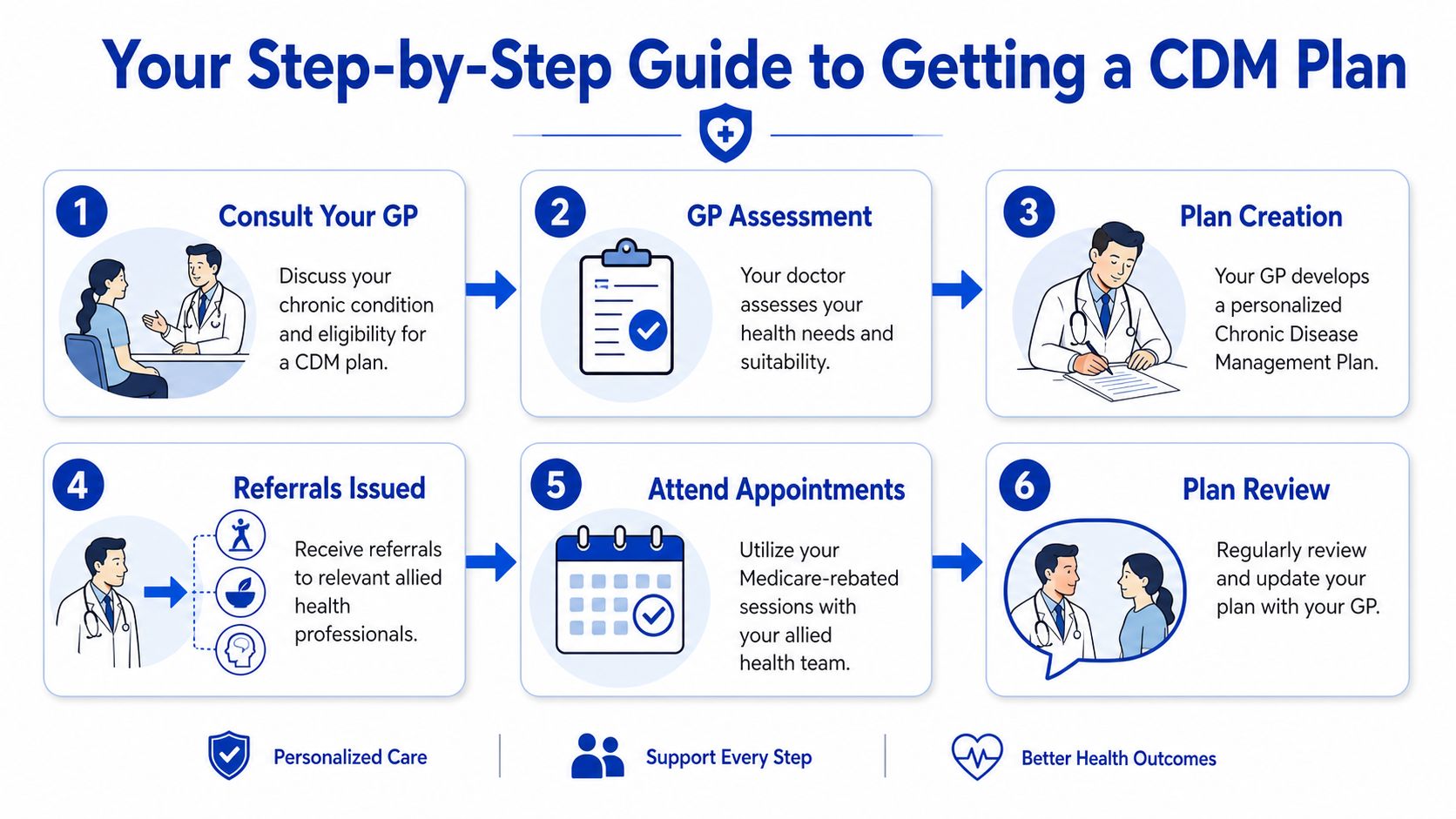
Step 1 Book a longer GP appointment
Don't book a standard quick visit if you already know you want to discuss chronic pain management. Tell reception you'd like an appointment to talk about a chronic condition plan or chronic disease management. That gives your GP enough time to assess the issue properly.
Step 2 Prepare what you want to say
Write down the basics before you go:
- How long it's been going on
- What it stops you doing
- What makes it flare
- What you've already tried
You don't need a speech. A short list on your phone is enough. Clear detail helps your GP judge whether the condition is chronic and whether allied health involvement makes sense.
Step 3 Discuss the condition in functional terms
This part matters. GPs don't only need a label. They need to understand impact.
Try language like:
- "My back pain has been there for months and it's affecting work and sleep."
- "My arthritis is making walking and stairs harder."
- "My neck pain keeps coming back and I want a better management plan."
Step 4 Let your GP build the plan
If your GP decides a plan is appropriate, they'll document the condition, your needs, and the allied health support that may help. From the patient's side, this is usually much less complicated than it sounds. The main task is answering questions clearly and making sure your goals are realistic.
A useful goal is "I want to walk more comfortably" or "I want fewer flare-ups at work." A less useful goal is "I want this fixed immediately."
Step 5 Receive your allied health referral
Once the plan is set up, your GP can issue the allied health referral connected to it. Since the process changed in 2025, the referral pathway is more straightforward than the older arrangement patients may have heard about.
When you receive the referral:
- Check which provider type you've been referred to
- Confirm how many visits are being allocated initially
- Ask how reviews will work if more coordination is needed
Step 6 Book and use the referral properly
When you contact the allied health clinic, tell them you have a chronic disease management referral. Bring any paperwork the clinic asks for, and mention the condition named in your plan.
The early sessions usually work best when you treat them as the start of a management process, not a one-off treatment. Expect assessment, some treatment, practical advice, and a plan for what you should do between visits.
How Bayside Osteopathic Health Supports Your Care Plan
For patients with chronic musculoskeletal pain, osteopathic care can fit naturally into a broader management plan. That matters because chronic pain often isn't just about a single painful structure. It usually involves stiffness, movement compensation, muscular guarding, reduced confidence in activity, and habits that keep the problem simmering.

Medicare data shows a real gap here. Despite musculoskeletal conditions being explicitly eligible, chronic disease management plans are often under-utilised for linking patients to non-drug pain management options like osteopathy, as discussed in the AIHW chapter on allied health items and chronic disease management.
Where osteopathic care adds value
Osteopathic treatment is often helpful when the goal is to improve how your body moves and tolerates daily activity. In practice, that may involve:
- Hands-on treatment: Such as soft-tissue work, joint articulation, and gentle mobilisation
- Movement advice: Simple changes to reduce aggravation at work, at home, or during exercise
- Functional thinking: Focusing on what you need to do more comfortably, not only where it hurts
A visual like this hands-on treatment setting in clinic captures the kind of practical, person-to-person care many patients are looking for when pain has become persistent.
{kind=link}
What tends to work better than passive care alone
The best results usually come when hands-on treatment is part of a bigger plan. A few sessions may help settle pain and improve mobility, but long-term change often depends on what happens between visits as well. That includes pacing, posture changes, activity modification, walking, strengthening, and realistic flare-up management.
What doesn't work as well is treating chronic pain like an acute sprain that should disappear after one appointment.
For ongoing pain, the aim is usually steadier movement, better function, and fewer setbacks. Relief matters, but so does building confidence in your body again.
Why coordinated care matters
When osteopathic care sits inside a GP-managed plan, everyone has a clearer framework. The referral is linked to a recognised chronic condition. Treatment has a clinical purpose. Progress can be reviewed in context.
For patients, that often feels less scattered. Instead of trying random things in isolation, care becomes more deliberate. That's a major reason Medicare chronic disease management can be so useful when pain has stopped being a short-term issue.
Frequently Asked Questions About CDM Plans
Can I split my visits across different allied health providers
Usually, yes, if that fits your GP's plan and referrals. A patient with arthritis, for example, might use some visits for physical care and another visit for a different allied health need related to the same broader condition picture. The exact referral arrangement should be clarified with your GP.
Do I have to use the provider my GP suggests
You can ask whether you may attend your preferred allied health provider. Patient choice matters, and the more simplified referral process introduced from July 2025 makes that easier in practical terms. If you already trust a particular clinic, mention that during the GP appointment.
Will five visits be enough
Sometimes they help a lot. Sometimes they mainly get the process started. For long-standing pain, the rebate is often best viewed as support for initial management rather than complete care. Its primary value is that it lowers the barrier to starting treatment and getting a proper plan in place.
What if my condition changes
Tell your GP. Chronic conditions can improve, flare, or become more complicated over time. Your plan should reflect what's happening, not what was true months ago.
Can osteopathy be relevant if my pain isn't severe every day
Yes. Chronic pain doesn't have to be constant to matter. Recurring flare-ups, stiffness, reduced mobility, and activity limits can still justify a proper management discussion if the condition is ongoing and allied health care may help.
What should I bring to my first allied health appointment
Bring your referral, any relevant scan reports if you have them, a medication list if it helps explain your situation, and a simple summary of what aggravates or eases your symptoms. You don't need to prepare perfectly. Clear information is enough.
If you'd like help understanding whether your referral may apply to osteopathic treatment, Bayside Osteopathic Health offers gentle, hands-on care for ongoing back, neck, and joint pain, and can help you understand the practical next steps for using a chronic disease management referral well.