You wake with a headache that sits behind one eye or wraps from the base of your skull to your temple. It isn't the dramatic, pounding kind people usually call migraine. It's just there. Nagging. Familiar. Often worse after a day at the desk, a long drive, or a poor night's sleep. You rub your neck and realise the pain seems to start there.
That pattern is more common than many people think. A lot of people live with “headaches” that are at least partly driven by the neck, but they never get a clear answer because the symptoms overlap with migraine, tension-type headache, jaw tension, and posture-related strain. When painkillers only dull it, or don't touch it at all, it's easy to feel stuck.
A cervicogenic headache refers to a headache with a neck problem at its root. The encouraging part is that when the neck is the true underlying cause, treatment can be very practical. It often involves improving movement, calming irritated tissues, and rebuilding neck function rather than just chasing symptoms.
Good cervicogenic headache treatment starts with the right diagnosis. That's where a skilled practitioner matters most. If the pain is coming from your neck, hands-on assessment can be very revealing. If it isn't, or if there's a mixed picture, that needs to be recognised early too.
Table of Contents
- That Nagging Headache Might Be Coming from Your Neck
- Understanding Cervicogenic Headaches
- How a Cervicogenic Headache is Diagnosed
- Evidence-Based Cervicogenic Headache Treatment
- Your At-Home Care Plan for Neck and Headache Relief
- Red Flags and When to Seek Specialist Care
- How Bayside Osteopathic Health Can Guide Your Recovery
That Nagging Headache Might Be Coming from Your Neck
A common story goes like this. The pain begins low, near the top of the neck, then creeps upward into the back of the head and settles on one side. By afternoon, turning your head feels stiff. You try rest, water, stretching, maybe over-the-counter medication. Sometimes it eases. Often it lingers.
That's the sort of presentation that makes clinicians think about the neck as a contributor. Not every headache with neck pain is cervicogenic. Migraine can cause neck discomfort too. Tension-type headache can make the neck feel tight. Jaw problems can also muddy the picture. Still, when the pain pattern is repeatable and tied to neck posture or movement, the neck deserves a proper look.
Why this matters early
People often spend months treating the wrong thing. They may assume every one-sided headache is migraine, or that every “tight band” headache is stress. The problem with guessing is simple. Different headache types respond to different treatments.
Practical rule: If a headache keeps returning with neck stiffness, reduced neck movement, or pain triggered by certain positions, don't ignore the neck.
Cervicogenic headache treatment is usually most effective when it's built around cause, not just symptom relief. That means asking better questions. What movements bring it on? What positions aggravate it? Is the pain reproducible when the neck is examined? A skilled osteopath, physio, GP, or headache clinician should be able to sort through that with you.
Understanding Cervicogenic Headaches
What cervicogenic means
Cervicogenic means “coming from the cervical spine,” which is your neck. In this type of headache, the pain is felt in the head, but the source is in cervical joints, muscles, or related structures. This is similar to a wiring issue in one room causing a light to flicker in another. The head hurts, but the irritation starts lower down.
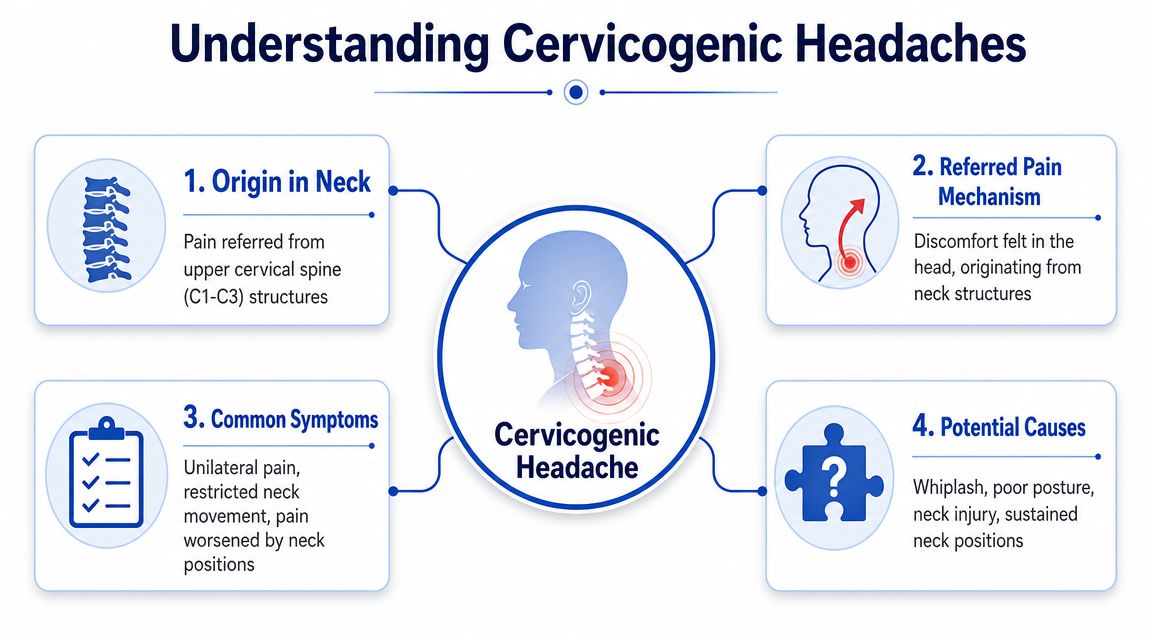
This is why the headache can feel confusing. The pain is real and localised to the head, yet treatment aimed only at the head often misses the true driver. When upper neck structures become irritated or don't move well, they can refer pain upward into the skull, temple, eye region, or behind the ear.
The symptoms that often point to the neck
The classic pattern is a headache that feels linked to neck dysfunction. Not everyone reads like a textbook, but several features raise suspicion.
- One-sided pain: The headache is often more dominant on one side and may stay on that side.
- Neck stiffness or reduced movement: Turning your head or looking up may feel restricted.
- Pain triggered by posture: Long hours at a screen, sleeping awkwardly, or sustained driving can flare it.
- Tenderness in the upper neck: Pressure through certain neck structures may reproduce familiar pain.
- A non-throbbing, mechanical feel: Many people describe it as aching, pulling, or pressure-like.
A bibliometric review noted a cervicogenic headache prevalence of 4.1% in one study set and highlighted manual therapy and randomised clinical trials as major research themes, which gives some context for how established this diagnosis is within the literature on conservative management (research synthesis on cervicogenic headache prevalence and treatment themes).
Why it gets confused with migraine and tension headache
Patients often find the distinctions challenging. Migraine can also be one-sided. Tension-type headache can coexist with neck tightness. Some people have more than one headache type at the same time. Consequently, a neck-focused explanation can be right, partly right, or wrong.
A particularly important unanswered question is whether neck-focused treatment is enough when the diagnosis is uncertain. Australian-facing information often frames cervicogenic headache as a neck problem, but it doesn't clearly tell patients how often they may have mixed headache disorders. PM&R KnowledgeNow notes that confirmatory blocks are recommended in some cases, which underlines why diagnostic accuracy matters before care is escalated (guidance on diagnosis and confirmatory blocks in cervicogenic headache).
The biggest mistake isn't having neck pain with a headache. It's assuming the neck is the whole answer without testing that assumption.
A good assessment doesn't just ask, “Does your neck hurt?” It asks whether your symptoms behave like a neck-driven headache, a migraine pattern, a tension pattern, or a blend of more than one.
How a Cervicogenic Headache is Diagnosed
What a skilled assessment looks for
Diagnosis usually starts with a detailed history. The timing matters. So does the pain path. A practitioner will want to know whether the headache starts in the neck, whether it stays on one side, which movements provoke it, and whether there's a link with work posture, sleep position, previous injury, or jaw clenching.
The physical exam is just as important. In a hands-on assessment, the clinician checks neck range of motion, muscle tone, joint irritation, posture, and whether pressure or movement in specific areas reproduces your familiar headache. That last part matters. Reproducing a known pain pattern through the neck gives useful clinical clues.
A careful exam often includes:
- Movement testing: Looking at rotation, extension, side bending, and combined neck movements.
- Palpation: Checking for tenderness and tissue tension around the upper neck and base of the skull.
- Postural assessment: Not to blame posture for everything, but to see whether habitual loading is contributing.
- Screening for overlap: Looking for signs that suggest migraine, tension-type headache, jaw involvement, or nerve irritation instead.
Why scans often play a limited role
Many patients assume they need an X-ray or MRI to “prove” a cervicogenic headache. In reality, imaging often has a more limited role. It can help rule out other conditions or investigate unusual features, but it doesn't always confirm the reason a headache is happening.
That's because pain from the neck can come from movement dysfunction and irritated tissues that don't show neatly on a scan. A normal scan also doesn't automatically mean the neck isn't contributing. This is one reason experienced clinical examination matters so much in cervicogenic headache treatment.
A scan can support a diagnosis or exclude something more serious. It rarely replaces a thorough hands-on assessment.
When diagnostic uncertainty changes the plan
Not every patient should follow the same path. If the pattern strongly fits a mechanical, neck-driven headache, conservative care is often a sensible first step. If the presentation is mixed, unusual, or not responding as expected, the plan changes.
Here's a practical approach:
| Clinical picture | What it often means |
|---|---|
| Clear neck trigger, reproducible pain, restricted neck movement | Trial of conservative neck-focused care is reasonable |
| Headache with strong migraine features as well | Mixed presentation may need shared management with GP or specialist |
| Symptoms don't behave mechanically | Reassess the diagnosis rather than pushing harder on the neck |
| Persistent uncertainty | Consider GP review and possible specialist referral |
A skilled practitioner's expertise is evident not only in treatment, but in knowing when a patient is a good fit for manual care, when they need co-management, and when the neck may be only one piece of the picture.
Evidence-Based Cervicogenic Headache Treatment
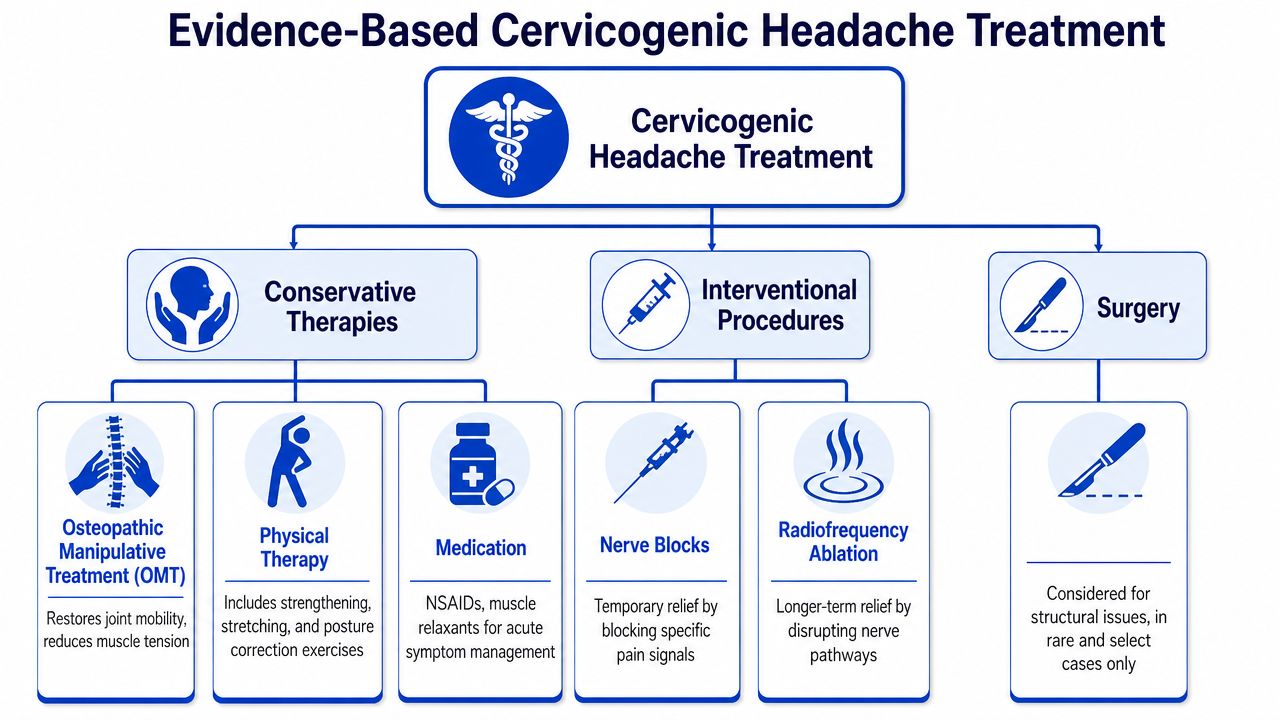
The strongest conservative approach isn't a single technique. In Australia, evidence supports a multimodal approach. A 2026 meta-analysis of 41 trials found that combining manual therapy with exercise produced the largest reductions in headache intensity, frequency, and disability, and an expert-panel guideline also recommends physical therapy and cervical manipulation as first-line management for long-term relief (evidence supporting multimodal cervicogenic headache treatment).
That matters because many people still look for one magic fix. One massage. One adjustment. One tablet. In practice, the people who do best usually have a plan that combines symptom relief with movement restoration and self-management.
Manual and osteopathic therapy
Hands-on care can reduce irritation and improve neck movement when the right tissues and joints are involved. In osteopathic treatment, that may include soft-tissue work, gentle articulation, mobilisation, and careful treatment of surrounding muscles through the neck, upper back, jaw, and shoulder girdle where relevant.
The point isn't to “crack” your neck into place. The point is to calm sensitised structures and restore more normal movement so the neck stops feeding pain upward. Some patients respond best to very gentle work. Others tolerate more direct mobilisation. The technique should fit the patient, not the other way around.
Exercise and rehabilitation
Manual therapy helps open the door. Exercise helps keep it open.
Research and guidelines support a treatment model that targets cervical dysfunction directly. An expert-panel guideline recommends physical therapy as the preferred initial treatment, with cervical manipulation or mobilisation also recommended, and notes that physical therapy provides the most long-term relief by reducing nociceptive input from cervical structures (expert-panel guidance on first-line cervicogenic headache care).
That usually means building capacity in the deep neck flexors, upper quarter muscles, and postural support system rather than doing random stretches from the internet. If you're trying to understand how hands-on care and rehab differ, this comparison of osteopathy and physiotherapy approaches can help you see how each may fit into your plan.
Posture and ergonomic changes
Posture isn't a diagnosis, but sustained loading can keep a sensitive neck irritated. The aim isn't to sit like a mannequin. It's to reduce the amount of time your neck gets stuck in the same stressed position.
Useful changes often include:
- Screen height: Bring the top of the monitor closer to eye level so you're not poking your chin forward all day.
- Frequent resets: Break static posture with short movement intervals rather than waiting until you're stiff.
- Arm support: If your shoulders are constantly raised at the keyboard, your upper neck usually pays for it.
- Driving position: Bring the seat and mirrors to you, so you're not reaching with your head.
Medication and its limits
Medication can have a place, especially when pain is flared and sleep is poor, but it usually isn't the full answer for a neck-driven headache. PM&R KnowledgeNow notes that treatment typically starts with physiotherapy and medication before injections or surgery, while other reviews also point out that common pain relievers may have limited evidence in this setting. That's why cervicogenic headache treatment usually works better when medication is used as support rather than as the centrepiece.
For patients, the practical takeaway is simple. If medication keeps you functional while you address the neck properly, that can be useful. If medication is your only strategy and the headache keeps returning, the plan probably needs to change.
When interventional care is considered
Some people do need more than conservative care. That doesn't mean they've failed treatment. It means the diagnosis may need refining or the pain source may need to be tested more directly.
Options sometimes considered after appropriate assessment include image-guided diagnostic blocks and other interventional procedures. These are generally reserved for cases with persistent symptoms, diagnostic uncertainty, or poor response to conservative treatment. They can be particularly useful when the question isn't just “How do we treat this?” but “What is generating the pain?”
Conservative care should be active and time-limited. If you're not improving, the next step is reassessment, not endless passive treatment.
Your At-Home Care Plan for Neck and Headache Relief
The most useful home plan is the one you'll do. It doesn't need to be complicated. In fact, a simple routine done consistently usually beats an ambitious program abandoned after three days.

A structured 6-week program combining manual therapy with home exercise has been reported as effective in the short term and at one-year follow-up, with reduced headache symptoms and reduced medication intake, which supports the value of active self-care alongside treatment (summary of the six-week manual therapy and exercise program).
The home routine that usually helps most
Try these movements gently. None of them should create sharp pain, dizziness, or a marked increase in your headache.
Chin tucks
Sit tall and look straight ahead. Gently draw your chin backward, as if making a soft double chin. Don't tip your head up or down. Hold briefly, then relax. This helps switch on the front-of-neck support muscles that often become lazy when the head sits forward.Gentle neck rotation
Turn your head slowly to one side within a comfortable range, then return to centre and repeat to the other side. Keep the movement smooth. Don't force the end range. The goal is to restore easy motion, not win a stretching contest.Shoulder blade set
Let your shoulders relax. Then gently draw your shoulder blades slightly back and down. Hold briefly without arching your lower back. This can reduce the upper-neck workload that builds during desk tasks.
If you'd like extra guidance, these neck pain relief exercises show the kind of simple movement work often used to support recovery.
Simple daily habits that reduce flare-ups
Daily habits matter because neck-related headaches often build gradually.
- Use movement snacks: Stand, walk, or reset your neck regularly during screen work.
- Check your pillow: Aim for a pillow height that keeps your head reasonably level rather than sharply bent.
- Avoid repeated self-cracking: It may give temporary relief, but it often doesn't solve the underlying control problem.
- Respect the flare pattern: If one position always triggers symptoms, change the setup before blaming your body.
This video can help you visualise calm, controlled neck movement rather than aggressive stretching.
Consistency matters more than intensity. Gentle, regular movement usually settles a sensitive neck better than occasional forceful stretching.
A good home program should feel manageable. If it repeatedly aggravates your symptoms, the answer isn't to push harder. It's to adjust the plan.
Red Flags and When to Seek Specialist Care
Most neck-related headaches aren't emergencies, but some headaches need urgent medical attention. Don't try to self-manage these.
Seek immediate medical care if you develop:
- A sudden, severe headache: Especially one that peaks very quickly and feels unlike anything you've had before.
- Headache with fever and marked neck stiffness: This needs urgent medical assessment.
- Headache after a significant head or neck injury: Even if symptoms seem delayed.
- Neurological symptoms: Weakness, facial droop, confusion, fainting, difficulty speaking, new numbness, or major visual change.
- A clearly escalating pattern: Headaches that are rapidly worsening or accompanied by concerning new symptoms.
There's also a non-urgent specialist pathway. If a headache doesn't respond to appropriate conservative care, if the diagnosis remains muddy, or if migraine features are prominent alongside neck pain, a GP may refer you to a neurologist, pain specialist, or another clinician for further work-up.
The key point is this. Persistent headache deserves respect. If the pattern doesn't fit, if treatment isn't helping, or if the story changes, reassessment is the safest next move.
How Bayside Osteopathic Health Can Guide Your Recovery
When someone presents with a suspected cervicogenic headache, the first job is to work out whether the neck is primarily causing the pain, partly contributing, or merely becoming tense because another headache type is present. That distinction changes everything. It affects treatment choice, referral decisions, and what you should expect from care.

At Bayside Osteopathic Health services, care is built around that kind of musculoskeletal assessment. An osteopathic consultation can include examining neck movement, tissue tension, posture, upper back mechanics, and other factors that may be maintaining the problem. Treatment may involve gentle soft-tissue work, joint articulation, mobilisation, movement advice, and a home plan that supports recovery between visits.
This approach suits cervicogenic headache treatment because the goal isn't only to reduce pain in the moment. It's to improve how the neck functions, make flare-ups less likely, and recognise early when the presentation doesn't fit a straightforward neck-driven pattern.
For local patients, practical guidance also matters. That includes help understanding when GP involvement is useful, when specialist referral may be sensible, and whether Medicare support may apply through a Chronic Disease Management plan arranged by your GP if you're eligible.
If your headache seems to keep tracing back to your neck, a careful assessment can give you more clarity than guesswork ever will.
If you're ready to get clearer on whether your headache is neck-related, Bayside Osteopathic Health can help with assessment, gentle hands-on care, and a practical treatment plan that fits your symptoms and daily life.