A lot of people start looking for a cortisone injection in Perth when pain has stopped being a nuisance and started changing daily life. Your shoulder hurts every time you reach overhead. Your knee swells after a short walk. Your hip stiffens during the drive to work and then nags all afternoon. By the time you're searching, you usually don't want theory. You want to know what will help, how fast, and whether it's the right move.
Cortisone injections can be useful. They're also commonly misunderstood. Some people see them as a quick fix. Others worry they're dangerous and should always be avoided. The truth sits in the middle. For the right problem, at the right time, a cortisone injection can calm inflammation and give you a chance to move more comfortably again. But it doesn't automatically solve the reason the pain started.
That bigger picture matters. If your sore neck, shoulder, hip or knee is tied to load, posture, movement habits, training errors, work demands, or underlying joint change, then the injection is only one part of the answer. If you're also dealing with upper body tension, these neck pain relief exercises can be a useful example of how movement work often needs to sit beside pain relief, not after everything else has failed.
Table of Contents
- Struggling with Joint Pain in Perth?
- How a Cortisone Injection Fights Pain
- The Injection Procedure What to Expect
- Weighing the Benefits Against the Risks
- Making an Informed Choice Alternatives and Your Long-Term Strategy
- Frequently Asked Questions
Struggling with Joint Pain in Perth?
You wake up with a shoulder that catches when you reach for a shirt, or a knee that stiffens after the drive to work. By the end of the week, you are changing how you move without even realising it. You stop training, sleep poorly, and start wondering whether you need a scan, an injection, or just more time.
That is the point where many Perth patients ask about cortisone. It often comes up after a flare that has not settled, or when pain is blocking work, exercise, or basic daily tasks. The key thing to understand early is that a cortisone injection is usually a short-term tool. It may reduce pain enough to help you function, but it does not explain why the joint became irritated in the first place or what will stop it coming back.
That bigger picture matters. A painful neck, shoulder, hip, or knee rarely affects one structure in isolation. It changes how you load nearby joints, how well you sleep, and how confident you feel using the area again. If neck pain is part of the problem, simple neck pain relief exercises can be one part of a broader plan while you work out whether an injection is even needed.
In practice, the useful question is not “should I get a cortisone injection?” on its own. Ask, “what is this injection helping me do next?” For some people, the answer is getting pain low enough to start rehabilitation properly. For others, it is buying relief for a short period during an acute flare. And for some, it is not the right fit at all, especially if the main issue is poor joint loading, reduced strength, stiffness, or a pattern that keeps aggravating the tissue.
I want patients to see cortisone in context. It can be helpful. It can also disappoint when it is treated as the whole plan. The best decisions usually come from matching the injection, or the decision to avoid one, to the diagnosis, the stage of the problem, and the rehabilitation you are prepared to follow through with afterward.
That is where osteopathy can add value. Hands-on treatment, movement assessment, exercise advice, and load management do not replace every injection, and injections do not replace good rehabilitation. Used thoughtfully, they can complement each other. Used in isolation, both tend to have limits.
How a Cortisone Injection Fights Pain
A cortisone injection aims to settle an irritated area so pain becomes more manageable. That can be useful if a shoulder has become too painful to reach overhead, or a knee flare is making walking difficult. The effect is usually about symptom control. It does not repair cartilage, restore strength, or correct the loading pattern that may have led to the problem.
What cortisone actually does
Cortisone is a corticosteroid medicine. When it is injected into a joint or around a painful soft tissue structure, the goal is to reduce local inflammation and calm the chemical irritation that is contributing to pain. If that response settles, swelling may ease, movement can feel less restricted, and everyday tasks often become more tolerable.
That short-term drop in pain can create a useful window.
For the right person, that window means sleeping better, walking with less guarding, or finally being able to start the exercises they were too sore to do before. In practice, this is often where the injection has the most value. It buys breathing room. What you do with that breathing room matters more than the injection itself.
Pain relief can also be misleading if it is treated as proof that the problem has been fixed. A tendon may still be under more load than it can handle. A stiff joint above or below the painful area may still be changing how you move. Reduced pain is helpful, but it is not the same as restored function.
Common problems it may be used for
Cortisone injections are commonly used for conditions where inflammation is thought to be part of the pain picture. Depending on the diagnosis and the structure involved, this can include:
- Shoulder pain involving an inflamed bursa or irritated surrounding tissues
- Knee pain where an arthritic or inflammatory flare is limiting movement
- Hip or trochanteric region pain linked with irritated soft tissues
- Elbow or wrist pain where there is a clear inflammatory target
- Arthritic flare-ups where short-term symptom relief may help day-to-day function
The key phrase is clear inflammatory target. If the main problem is compression, repeated overload, weakness, poor movement control, or a return to work or sport that outpaced tissue capacity, an injection may reduce symptoms for a period without changing the reason the area keeps flaring.
That trade-off is worth understanding before you book one. Good pain relief can be very helpful. It can also tempt people to do too much too soon, especially if they return to lifting, running, golf, or long workdays before strength and tolerance have improved.
From an osteopathic point of view, the best use of a cortisone injection is often as part of a broader plan. The injection may calm an irritated joint or tissue. Assessment, hands-on care, exercise advice, and load management help address the factors that keep provoking it. That is usually the missing piece behind the question patients ask after the injection works. What next?
The Injection Procedure What to Expect
Many people feel less anxious once they know what the appointment usually involves. The process is generally straightforward, but it's still helpful to know what happens before, during, and after the procedure.

Before the appointment
A cortisone injection is typically accessed through a GP, sports doctor, or specialist review. The first step should be a diagnosis, not just a painful body part. A clinician needs to decide whether inflammation is a meaningful part of the picture and whether an injection matches your symptoms, history, and examination findings.
In Perth, some injections are done in specialist rooms and many are performed in radiology settings, often with imaging guidance for accuracy. You'll usually be asked about medications, allergies, diabetes, recent illness, and whether you've had injections in that area before.
Bring practical questions with you, such as:
- What structure are you injecting? Ask for the exact joint or tissue target.
- What result should I expect? You want a realistic explanation, not just “it might help.”
- What will I do if it works? Rehab planning starts here.
- What if it doesn't help? A poor response can change the diagnosis or next step.
Costs and rebates vary by provider, referral pathway, and individual cover. Because fees differ between clinics and billing arrangements change, it's best to ask the clinic directly for itemised costs, whether there's a Medicare rebate in your situation, and whether private health applies.
During and after the injection
The actual procedure is often quick. The area is cleaned. A needle is placed into the target area, sometimes with local anaesthetic and sometimes with imaging guidance depending on the site and clinic setup. It is often described as uncomfortable rather than dramatic, though some areas are more sensitive than others.
You may then be asked to rest briefly before heading home. It's sensible to avoid planning a heavy gym session, long physical shift, or demanding sport immediately afterwards. A calmer day is usually the better choice.
A helpful visual overview of the process and patient experience is below.
During and after the injection
After the procedure, the key question is not “Do I feel amazing right now?” but “How does this area settle over the next few days?” Some people notice relief quickly. Others feel temporary soreness first and only later start to notice the intended benefit.
Mayo Clinic's clinical overview is noted in the verified brief as advising people to protect the area for 1 to 2 days after the shot and watch for infection signs. That advice is sensible in day-to-day practice as well. Don't use a pain drop as permission to go hard too soon.
The first pain-free day after an injection is not a fitness test. It's a chance to move more sensibly.
If you've had a cortisone injection in Perth and pain settles, that's the moment to review work set-up, training load, movement quality, sleep positions, strength deficits, and the habits that may have contributed in the first place. If you skip that step, the calm period can disappear quickly.
Weighing the Benefits Against the Risks
Cortisone injections stay popular for a simple reason. They can help. When the right tissue has been targeted and inflammation is a major driver, people may feel meaningful relief and regain enough movement to sleep better, walk more comfortably, or begin rehabilitation.
Why people choose it
The strongest argument for a cortisone injection is speed. If pain has become the main barrier to moving, then reducing that pain can change the whole treatment picture. Instead of being stuck in guarding, limping, or avoiding basic tasks, you may suddenly have enough comfort to restart normal movement.
That matters because rehab often fails when pain is too hot. If every exercise flares symptoms, patients lose confidence and stop. If a clinician can calm the area first, exercises, manual treatment, and activity modification often become more productive.
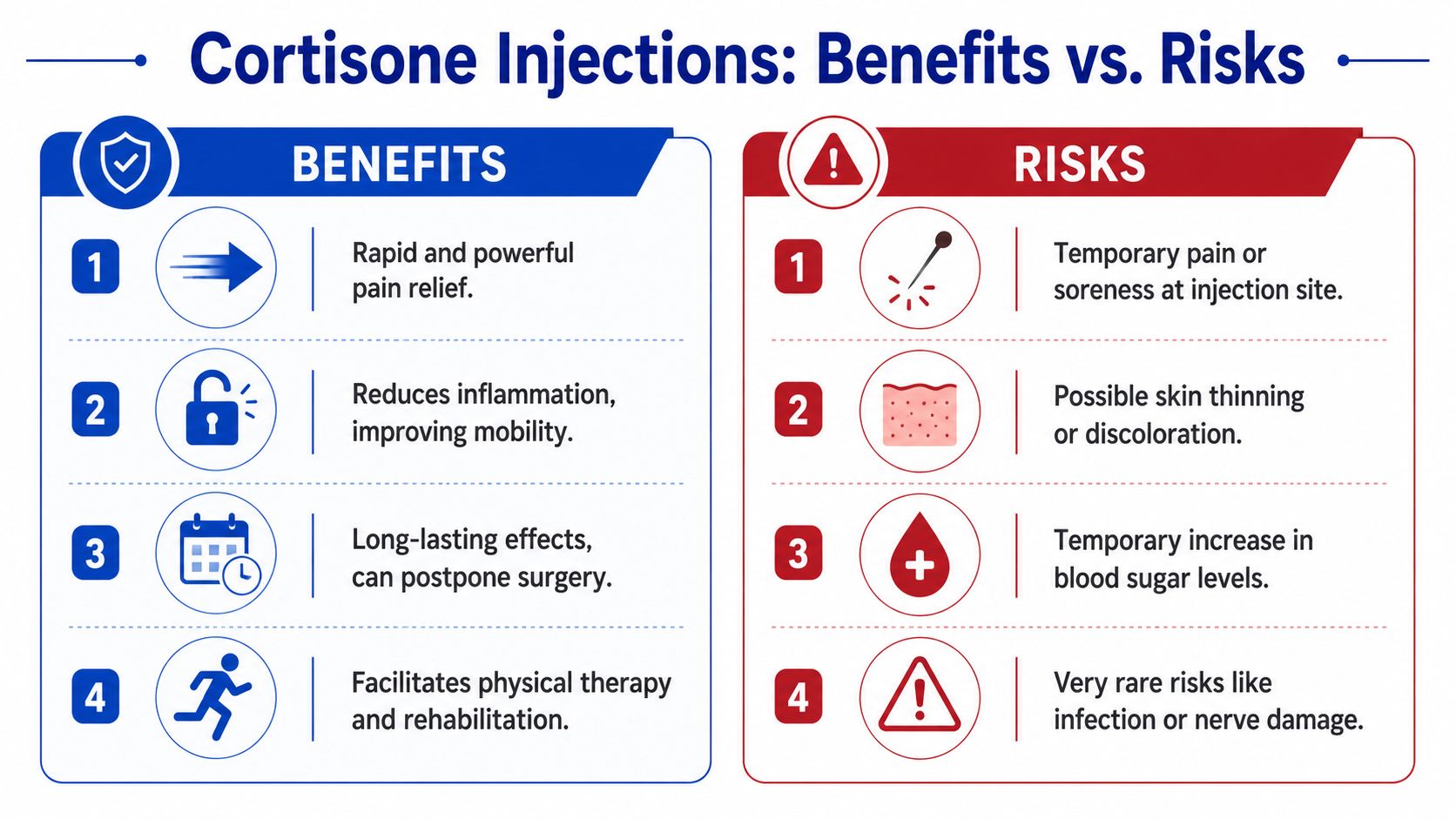
A useful way to think about the benefits is:
- Pain reduction: Less pain can improve sleep, walking, dressing, lifting, and work tolerance.
- Movement return: A calmer joint or tendon region often moves more freely.
- Rehab opportunity: Lower pain can make exercise and hands-on care easier to tolerate.
- Short-term support: It can help during a flare while a broader management plan is put in place.
Why clinicians still set limits
The fact that cortisone can help doesn't mean more is always better. The trade-off is cumulative exposure. Repeating injections too freely can increase the chance of local side effects and may encourage a cycle where symptoms are repeatedly suppressed without enough attention to the root cause.
According to Perth Radiological Clinic, while there is no scientifically proven absolute limit, clinicians generally permit only three cortisone injections into the same body part over 12 months. The same verified data notes this common-sense rule is used to help minimise issues such as post-injection flare, skin whitening, and the cumulative impact of the steroid on local tissues.
That doesn't mean the third injection is automatically wrong or the first is automatically right. It means clinicians need to ask better questions before repeating treatment.
Clinical judgment matters: If an injection gave short-lived relief but nothing changed in strength, function, or flare pattern, repeating it without a revised plan often isn't the smartest move.
You should also know that risk discussions aren't fear tactics. They're part of good consent. Minor soreness after the procedure can happen. More significant issues, such as infection, need prompt review. If you have diabetes, medication considerations, or a complex medical history, that should be part of the conversation before the needle goes in.
Making an Informed Choice Alternatives and Your Long-Term Strategy
Those searching for a cortisone injection in Perth aren't really searching for an injection. They're searching for a way to get their life back. They want to sleep, work, train, garden, commute, or move without thinking about pain all day.
That's why the bigger question is strategy. The verified brief highlights an important gap in patient guidance. Many people are seeking a long-term solution, but the benefits of an injection are often temporary, and it should sit inside a broader care plan. The same brief also notes that musculoskeletal conditions are a leading reason for GP visits in Australia, and many patients need clearer guidance on what to do if pain returns and when to prioritise exercise-based rehabilitation or manual therapy, as discussed on Perth Sports Medicine's cortisone injection page.
Use the injection as a window, not the whole plan
A useful mindset is to treat the injection as a window of opportunity. If pain settles, use that window well. Build strength. Improve joint motion. Change aggravating habits. Adjust training load. Address stiffness above and below the painful area. If your body moves better and tolerates load better, the chance of staying comfortable usually improves.
Approaches differ. Physiotherapy often leans heavily into targeted exercise progressions, load management, and tissue capacity. Osteopathy often combines hands-on treatment with movement advice and a broader look at how the whole body is sharing load. If you want a plain-English breakdown of those differences, this guide on osteopathy vs physiotherapy which is right for you is a helpful comparison.
Neither approach is about competing with injections. Both can work alongside them. In some cases, either option may help you avoid needing one.
Comparing Pain Management Approaches
| Approach | Cortisone Injection | Osteopathy | Physiotherapy |
|---|---|---|---|
| Main focus | Reducing inflammation in a targeted area | Improving movement, reducing tension, supporting whole-body mechanics | Restoring function through exercise, load management, and physical rehab |
| Best use | Painful inflammatory flare where short-term relief may help | When pain is linked with stiffness, posture, joint restriction, or compensations | When strength, capacity, tendon loading, or return-to-activity planning are central |
| What it may help with | Settling pain enough to resume daily tasks or rehab | Hands-on relief, mobility, body awareness, and movement confidence | Structured progression back to work, sport, and repeated loading |
| What it doesn't do well alone | It doesn't usually address long-term drivers by itself | It may not be enough if an inflammatory flare is too reactive | Exercise can be hard to tolerate if pain is too irritable at the start |
| How it fits a plan | Useful as one tool | Useful as part of broader conservative care | Useful as part of broader conservative care |
A good plan usually answers both questions. “How do we calm this down?” and “How do we stop it coming straight back?”
Questions worth asking before you repeat an injection
If the first injection helped but symptoms returned, don't automatically book the next one. Ask whether the broader plan changed anything meaningful.
Consider these questions:
- Did my function improve? Less pain matters, but better walking, sleeping, lifting, or training matters more.
- Did I use the calmer period well? If no rehab, no exercise progression, and no load change happened, the benefit may have been wasted.
- Has the diagnosis been reviewed? If response was poor, the original target may not have been the main driver.
- Am I treating a flare or chasing repeated relief? Those are different situations.
- What's the non-injection plan from here? You should be able to name it clearly.
From an osteopathic perspective, this is often where people get unstuck. They've had pain treatment, but they haven't had a full movement strategy. Their shoulder is quieter, but their upper back is still rigid. Their hip is less sore, but their gait, strength, or work setup hasn't changed. Their knee is better for now, but stairs and squats are still loaded poorly.
A cortisone injection can be an excellent short-term tool. It just shouldn't be the entire story.
Frequently Asked Questions
How long should I wait before deciding whether the injection worked?
Don't judge it too early. National guidance from earlier in this article notes that cortisone injections typically start working after a few days, not always immediately. Give it a bit of time, and track practical changes such as walking, sleep, dressing, reaching, stairs, or work tolerance rather than focusing only on raw pain.
What should I do in the first couple of days afterwards?
Keep things sensible. Protect the area, avoid heavy loading, and don't test it just because it feels a bit better. Gentle movement is usually more helpful than complete rest, but hard training, repetitive lifting, or long physical jobs straight away can irritate the area again.
What if the pain comes back?
Pain returning doesn't automatically mean the injection failed. It may mean the short-term anti-inflammatory effect has passed and the underlying issue still needs attention. That's the point to review diagnosis, exercise, movement habits, workload, recovery, and whether hands-on care or rehabilitation should become the main focus.
When should I think beyond another injection?
Think beyond another injection if relief was brief, if your function never really improved, or if you're repeating the same cycle without a better long-term plan. If you're looking for support with movement, joint stiffness, recurring flare-ups, or hands-on care, finding an osteopath near me can be a practical next step to explore.
If you're unsure, write down three things before your next appointment: what makes the pain worse, what improved after the injection, and what still hasn't changed. That gives your clinician something more useful than “it sort of helped”.
If you want a more detailed plan for ongoing joint, back, neck, or mobility issues, Bayside Osteopathic Health offers gentle, hands-on osteopathic care that looks beyond short-term symptom relief. Their approach focuses on how your body moves as a whole, with treatment, practical advice, and personalized self-care to help you move more comfortably and confidently.